Treatment
Focal Therapy
Focal therapy treats only the part of the prostate containing cancer. The rest of the gland, and the nerves and structures around it, are left intact.
What it is
Focal therapy is the targeted destruction of a prostate tumor using energy (cryoablation, HIFU, or laser ablation) under MRI/ultrasound guidance. It sits between active surveillance and whole-gland treatment and aims to control the cancer without the urinary and sexual side effects of radical prostatectomy or radiation. Dr. Rastinehad helped pioneer MRI-guided focal laser ablation and has been a principal investigator on multiple landmark focal therapy trials.
Best suited for
- Men with localized, MRI-visible, intermediate-risk prostate cancer (Gleason 3+4 or select 4+3).
- Patients prioritizing preservation of urinary continence and erectile function.
- Tumors confined to one region of the prostate on imaging and biopsy (unifocal or dominant index lesion).
- Men whose disease has progressed on active surveillance and who want to avoid whole-gland treatment.
- Select patients with recurrent cancer after radiation (salvage focal therapy).
How it works
- 1Multiparametric MRI (T2, diffusion, dynamic contrast) maps the tumor and assigns a PI-RADS score.
- 2An MRI-fusion biopsy confirms cancer location, grade, and rules out clinically significant disease elsewhere in the gland.
- 3Treatment plan is built to cover the tumor plus a 3 to 5 mm safety margin while protecting the urethra, sphincter, and neurovascular bundles.
- 4Energy (laser, cryo, or HIFU) is delivered to the tumor under live MRI or ultrasound guidance.
- 5Surveillance MRI at 6 to 12 months and a confirmatory biopsy of the treated area verify treatment success.
MRI-guided focal therapy, step by step
MRI mapping, then MRI/ultrasound fusion biopsy, then targeted ablation, then confirmatory follow-up MRI.
1. MRI mapping
Multiparametric MRI (T2-weighted, diffusion-weighted, ADC, and dynamic contrast enhancement) identifies the high-suspicion lesion and assigns a PI-RADS score so the tumor's location, size, and aggressiveness are clear before any intervention.
2. MRI/ultrasound fusion biopsy
Real-time transrectal ultrasound is fused with the diagnostic MRI so the biopsy needle is directed precisely into the suspicious lesion. This confirms cancer grade and rules out clinically significant disease elsewhere in the gland.
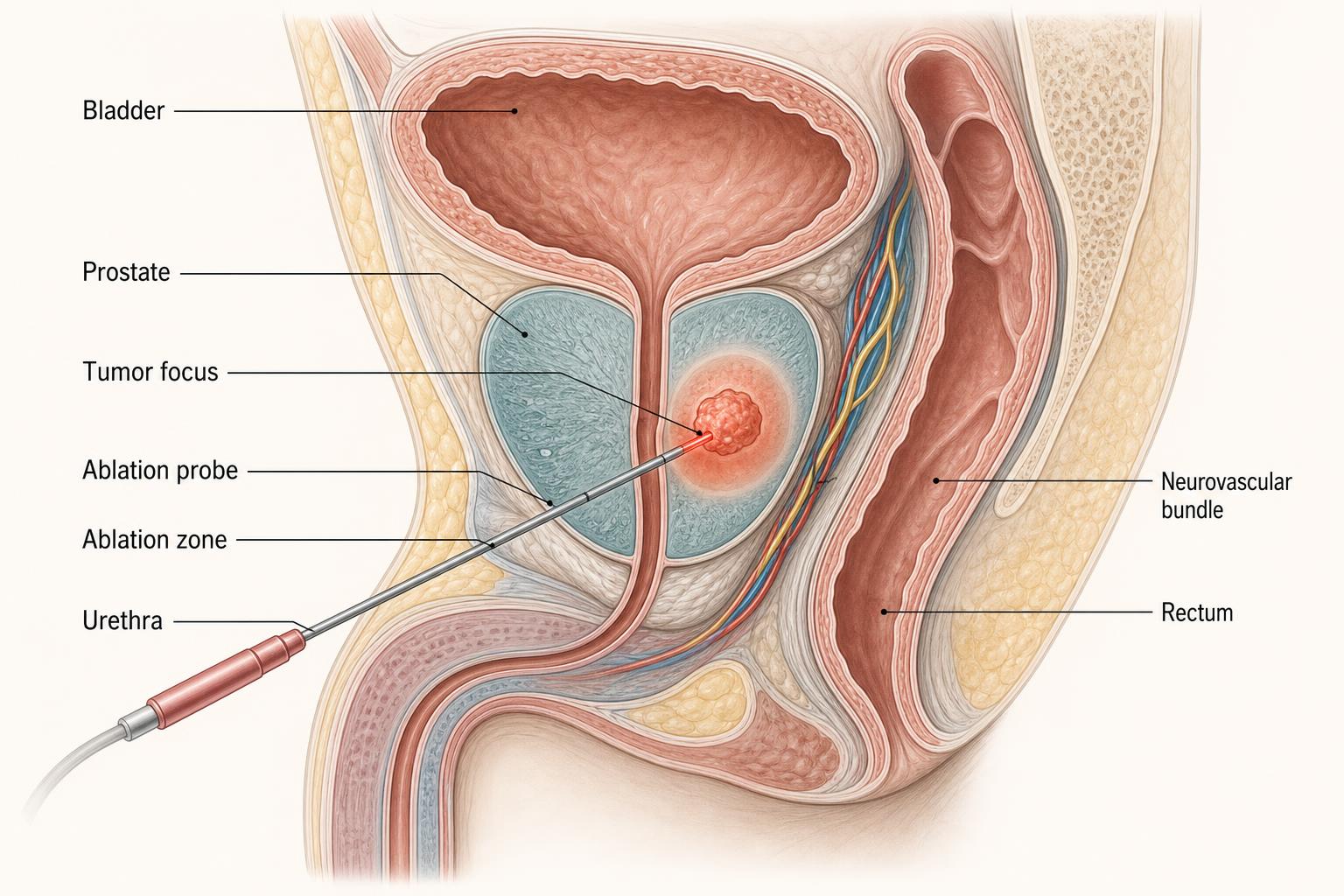
3. Targeted ablation
An ablation probe is placed through the perineum and energy (laser, cryo, or HIFU) is delivered to the tumor plus a 3–5 mm safety margin. The urethra, urinary sphincter, and neurovascular bundles are deliberately preserved.
4. Confirmatory follow-up MRI
Post-treatment MRI at 6–12 months shows the ablation zone (a healing scar), absence of residual high-suspicion lesion, and preserved healthy prostate tissue. A confirmatory biopsy of the treated zone is performed when indicated.
Benefits
- Markedly lower rates of incontinence and erectile dysfunction than whole-gland treatment.
- Preserves all future treatment options if they are needed (surgery, radiation, or repeat focal).
- Quick recovery and same-day discharge.
- Catheter typically removed within 1 to 3 days.
Possible risks
- Need for re-treatment in a subset of patients (typically 10 to 20%).
- Temporary urinary urgency, frequency, or retention.
- Less common: rectal irritation, urethral stricture, or perineal discomfort.
- Residual or recurrent cancer requires lifelong PSA and MRI surveillance.
Focal therapy vs. alternatives
| Radical prostatectomy | Definitive whole-gland removal. Higher rates of incontinence (5 to 20%) and ED (30 to 60%) even with nerve-sparing. |
|---|---|
| Radiation therapy | Effective whole-gland treatment. Bowel and urinary toxicity, and limits future salvage options. |
| Active surveillance | No treatment side effects, but progression risk persists and many men eventually need definitive therapy. |
Preparing for your procedure
- Recent multiparametric MRI and MRI-fusion biopsy results sent for review.
- Hold blood thinners as directed (typically 5 to 7 days).
- Bowel prep the evening before. Nothing by mouth after midnight.
- Arrange a ride home. No driving for 24 hours after anesthesia.
Why patients choose Dr. Rastinehad
Dr. Rastinehad was an early leader in MRI-guided focal therapy and MRI/ultrasound fusion technology. He has published extensively on focal laser ablation and has trained colleagues nationally and internationally in image-guided prostate cancer treatment.
Used to treat
Conditions Dr. Rastinehad treats with Focal Therapy.
FAQ
About Focal Therapy
Answers patients most commonly ask before their consultation.
Candidacy is based on MRI findings, biopsy grade and location, PSA, and prostate size. Dr. Rastinehad will personally review your imaging and pathology before recommending treatment.
Ready to talk?
Personalized urologic care begins with a conversation.
Schedule a consultation to review your imaging, lab work, and treatment options.