Treatment
Prostate Artery Embolization (PAE)
Prostate artery embolization (PAE) is an outpatient, non-surgical procedure that relieves BPH symptoms by shrinking the prostate from the inside.
What it is
PAE uses microscopic particles delivered through a tiny catheter to selectively block the arteries feeding an enlarged prostate. The gland shrinks over several weeks. No prostate tissue is cut, no urethral instruments are used, and the procedure preserves the muscles and nerves responsible for continence and ejaculation. PAE is performed by an interventional radiologist or urologist. Dr. Rastinehad combines deep urologic training with image-guided expertise.
Best suited for
- Men with moderate-to-severe BPH symptoms (IPSS ≥ 13) who want to avoid TURP, laser surgery, or Rezum.
- Patients with very large prostates (>80g, often >150g) where traditional surgery carries higher risk.
- Men prioritizing preservation of sexual function and antegrade ejaculation.
- Men on blood thinners or with cardiac comorbidities who are poor candidates for general anesthesia.
- Patients in urinary retention with an indwelling catheter who want to regain spontaneous voiding.
How it works
- 1Tiny puncture in the radial artery (wrist) or femoral artery (groin) under local anesthesia and light sedation.
- 2A microcatheter is navigated through the aorta and internal iliac arteries into the prostatic arteries using live fluoroscopy and CBCT mapping.
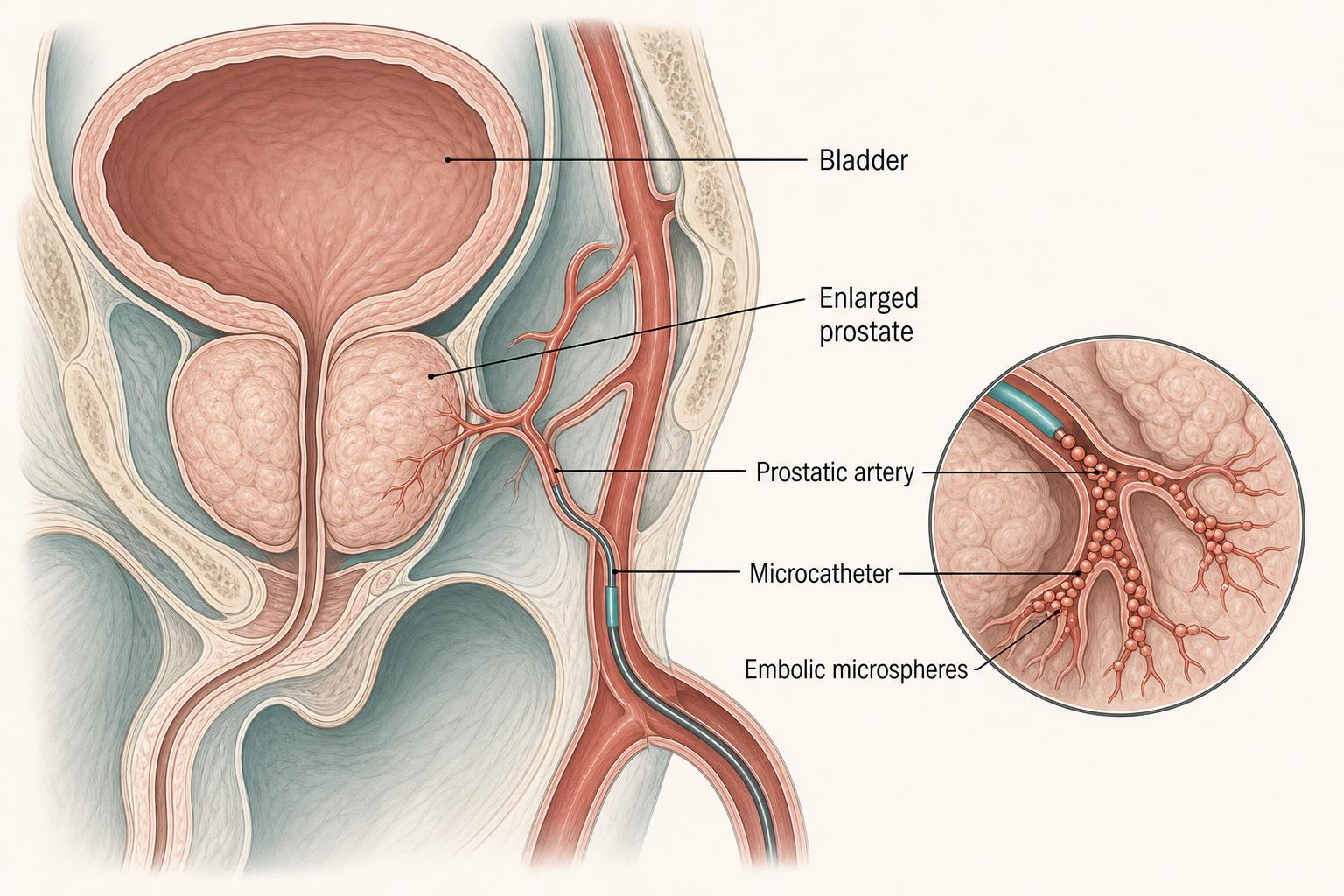
- 3Microscopic embolic particles (300 to 500 µm) are released to selectively block blood flow to the enlarged prostate tissue.
- 4Both prostatic arteries (left and right) are typically treated in the same session.
- 5Symptoms improve over 4 to 12 weeks as the gland infarcts and shrinks (typically 20 to 40% volume reduction).
Prostate artery embolization, step by step
Wrist access, then catheter navigation to the prostatic arteries, then microsphere embolization. The gland shrinks over the following weeks.
1. Radial artery access
Local anesthesia is given at the wrist and a 2 mm catheter is introduced into the radial artery. There is no groin puncture, no surgical incision, and no general anesthesia.
2. Navigation to the prostatic arteries
Under live X-ray guidance, a microcatheter is steered down through the aorta and into the small branches of the internal iliac arteries that feed the enlarged prostate.
3. Particle embolization
Calibrated microspheres are injected to selectively block blood flow to the prostate's enlarged tissue. Surrounding nerves, the urinary sphincter, and the ejaculatory mechanism are not disturbed.
4. Prostate shrinks and flow improves
Deprived of its blood supply, the prostate shrinks 20–40% over the following weeks. The urinary channel opens, urinary flow improves, and most men reduce or stop their BPH medications.
Benefits
- No risk of retrograde ejaculation, unlike TURP, Rezum, or UroLift.
- Preserved erectile and sexual function.
- No urethral catheter required for most patients after the procedure.
- Effective even for very large prostates (>80g) where other options are limited.
- Performed under local anesthesia with sedation. No general anesthesia required.
- Same-day discharge. Back to desk work within 2 to 3 days.
Possible risks
- Post-embolization syndrome (low-grade fever, pelvic discomfort, mild nausea) lasting 2 to 5 days, managed with NSAIDs.
- Mild bruising at the wrist or groin access site.
- Rare bladder or rectal wall irritation.
- Non-target embolization is uncommon with experienced operators (<1%).
- Approximately 10 to 15% of men may need a second PAE or alternative procedure over time.
PAE vs. other BPH procedures
| TURP (transurethral resection) | Gold-standard surgical option. Effective but has ~65% rate of retrograde ejaculation, requires hospital stay, longer catheterization, and general or spinal anesthesia. |
|---|---|
| Rezum (water vapor) | Office-based and preserves ejaculation in most patients. Best for prostates <80g. Requires catheter for 3 to 7 days and may need re-treatment. |
| UroLift | Best for smaller prostates without median lobe. Permanent implants. Less durable in very large glands. |
| Simple prostatectomy | Reserved for very large prostates. Major surgery with hospital stay and longer recovery. |
Preparing for your procedure
- Recent prostate MRI and uroflow on file. PSA reviewed to rule out cancer.
- Hold blood thinners as directed (usually 3 to 5 days before; some can continue).
- Light meal in the morning. Clear liquids only after.
- Arrange a ride home. No driving for 24 hours.
Why patients choose Dr. Rastinehad
Dr. Rastinehad is dual-trained in urology and interventional radiology. He is one of a small number of specialists in the U.S. who can both diagnose BPH urologically and perform PAE personally. Your evaluation, treatment, and follow-up are all delivered by the same physician.
Used to treat
Conditions Dr. Rastinehad treats with Prostate Artery Embolization (PAE).
FAQ
About Prostate Artery Embolization (PAE)
Answers patients most commonly ask before their consultation.
Most men notice symptom improvement within 2 to 4 weeks. Full benefit is typically reached by 3 months as the prostate continues to shrink.
Ready to talk?
Personalized urologic care begins with a conversation.
Schedule a consultation to review your imaging, lab work, and treatment options.