Treatment
Varicocele Embolization
Varicocele embolization is a minimally invasive, image-guided treatment for varicoceles, no incisions required.
What it is
A small catheter is guided through a vein in the neck or groin into the dilated internal spermatic (gonadal) vein. The refluxing vein is sealed off using platinum coils ± a sclerosant, and blood naturally reroutes through healthy collateral veins. The testicle continues to drain, only the abnormal refluxing pathway is closed. No incision, no scalpel, and no general anesthesia. Success rates and fertility outcomes are equivalent to or better than open or laparoscopic surgical ligation, with faster recovery and less pain.
Best suited for
- Men with symptomatic varicoceles (scrotal pain, heaviness, or swelling worse with standing).
- Couples with male-factor infertility and abnormal semen analysis linked to a varicocele.
- Adolescents and young men with documented testicular volume loss on the affected side.
- Patients with recurrent or persistent varicocele after prior surgical ligation.
- Anyone seeking a no-incision, no-general-anesthesia alternative to microsurgical varicocelectomy.
How it works
- 1Local anesthesia at a small puncture in the right internal jugular vein (neck) or right femoral vein (groin).
- 2A diagnostic venogram confirms the anatomy and identifies all refluxing channels.
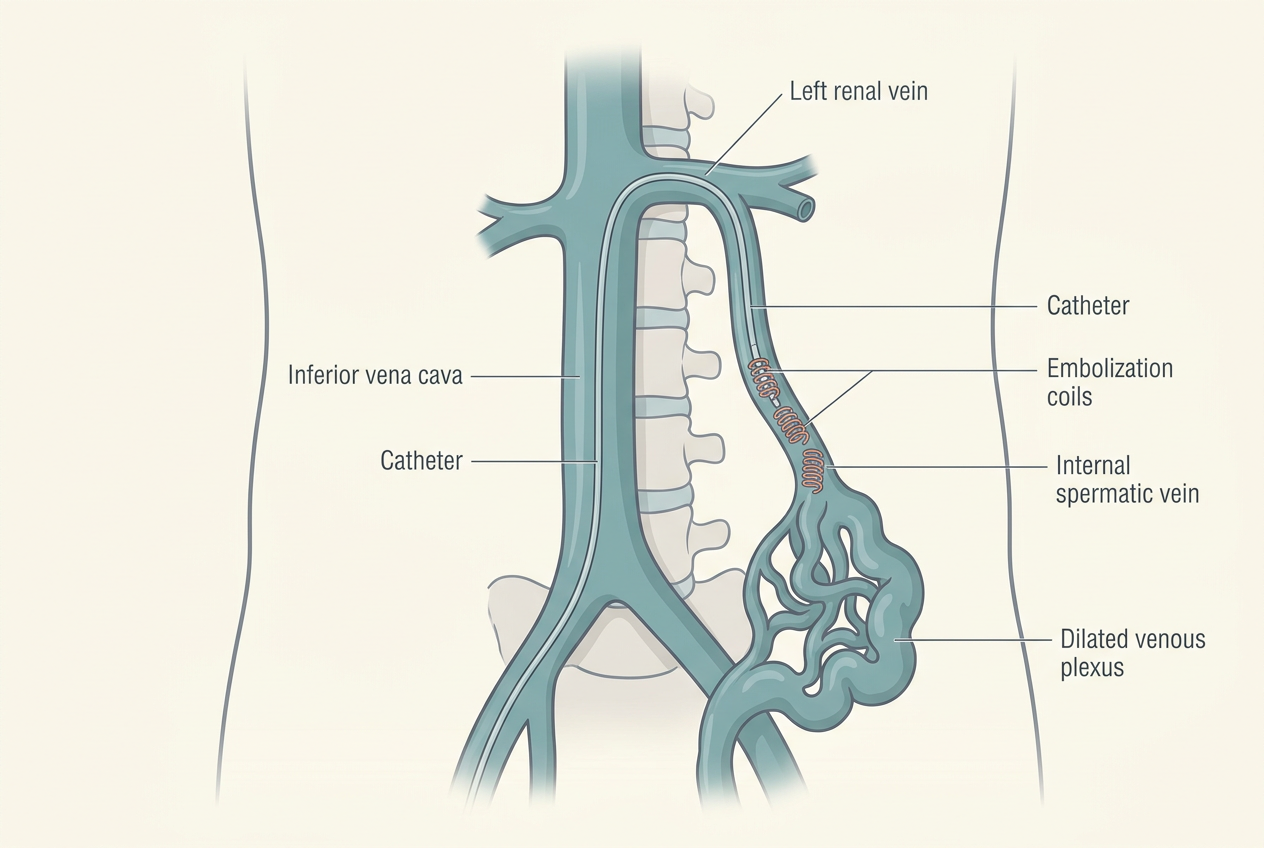
- 3A microcatheter is navigated through the inferior vena cava into the left (or right) spermatic vein.
- 4Platinum coils, sometimes combined with a sclerosing agent, are deployed to permanently close the abnormal vein.
- 5The catheter is removed and the access site closed with a small adhesive dressing. No stitches.
Varicocele embolization, step by step
Neck access, catheter advanced into the spermatic vein, platinum coil embolization, varicocele decompresses.
1. Jugular vein access
A small puncture is made in the right internal jugular vein in the neck under local anesthesia. No scrotal incision, no scalpel, and no general anesthesia.
2. Microcatheter navigation
Under live X-ray guidance, a thin microcatheter is steered through the vena cava and into the refluxing left (or right) internal spermatic vein. A diagnostic venogram confirms every abnormal channel.
3. Coil deployment
Platinum coils, sometimes combined with a sclerosing agent, are placed to permanently close the abnormal refluxing vein. Healthy collateral veins continue to drain the testicle normally.
4. Varicocele decompresses
With the refluxing pathway sealed, the varicocele decompresses. Scrotal heaviness and pain improve, scrotal temperature normalizes, and semen parameters typically improve over 3–6 months.
Benefits
- No incision, no scalpel, no sutures, small adhesive dressing only.
- No general anesthesia required; light IV sedation and local numbing.
- Faster recovery than open or laparoscopic ligation (back to desk work in 1–2 days, vs. 1–2 weeks for surgery).
- Equivalent or better success rates than surgical ligation in published series.
- Bilateral varicoceles treated in the same single session.
- Lower risk of hydrocele formation compared with surgical ligation.
- Both testicles continue to drain normally, only the abnormal vein is closed.
Possible risks
- Mild bruising or tenderness at the small access site (neck or groin).
- Brief lower-back or flank discomfort for 1–2 days (related to the embolic agent).
- Rare allergic reaction to contrast dye.
- Recurrence or persistence (5–10%), sometimes requiring a repeat embolization.
- Very rare coil migration (treated technique-dependently).
Embolization vs. surgical ligation
| Microsurgical varicocelectomy | Gold-standard surgery; requires inguinal/sub-inguinal incision, general or spinal anesthesia, 1–2 weeks off work, small risk of hydrocele or testicular artery injury. |
|---|---|
| Laparoscopic ligation | Requires general anesthesia, abdominal port incisions, longer recovery, higher hydrocele rate than embolization. |
| Open ligation (Palomo) | Higher recurrence and hydrocele rates than microsurgery or embolization; rarely first-line today. |
| Observation | Reasonable for asymptomatic varicoceles with normal semen analysis and no testicular volume loss. |
Preparing for your procedure
- Send recent scrotal ultrasound and (if applicable) semen analysis for review.
- Hold blood thinners as directed (typically 2–5 days; many can continue).
- Light meal in the morning; clear liquids only 2 hours before.
- Arrange a ride home; no driving for 24 hours after sedation.
Why patients choose Dr. Rastinehad
Dr. Rastinehad has performed hundreds of varicocele embolizations and trains other physicians in the technique. His urologic background means he understands the fertility, hormonal, and pain considerations driving treatment, not just the catheter work.
Used to treat
Conditions Dr. Rastinehad treats with Varicocele Embolization.
FAQ
About Varicocele Embolization
Answers patients most commonly ask before their consultation.
60–70% of men with male-factor infertility see improvements in sperm count, motility, or morphology within 3–6 months. Spontaneous pregnancy rates of 30–40% within a year are reported in published series.
Ready to talk?
Personalized urologic care begins with a conversation.
Schedule a consultation to review your imaging, lab work, and treatment options.